
 00389 2 3091 484
00389 2 3091 484
00389 2 3091 484
Life treatening surgery for mycotic aneurysm
јануари 15, 2014
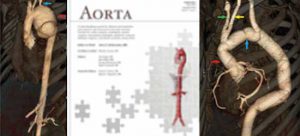
Life treatening surgery for mycotic aneurysm
Во новиот број на медицинското списание Аорта отпечатен е трудот на темаLife treatening surgery for mycotic aneurysmZan K Mitrev MDFETCS, Tanja N Anguseva MD
Едиторот го даде следново мислење за текстотEDITOR’S COMMENTS AND QUESTIONSEditor’s Comment:The authors are to be commended for advancedheroic treatment of a very challenging case. Furthermore,this case is valuable as an illustration of subsequentcare beyond the original operation.Editor’s Questions:1. Were the blood cultures positive? Were aortictissue cultures positive? Were bacteria seen inthe surgical specimen?We did not isolate positive blood cultures from thispatient. Aortic tissue cultures were also negative.But according to the literature, in 60%–70% of patients,blood cultures are negative, and even in theaortic tissue, cultures are negative in 25% of cases[1].The diagnosis of an infected aneurysm was establishedby clinical and operative findings, includingpathological findings of the aortic wall [with pathohistologicalreport, mycotic (infective) etiology ofthe aneurysm was confirmed, resulting in compressedperivascular tissue, hematoma, and fibroinflammatorytissue with plenty of polymorphonuclears].Essentially, three mechanisms of mycoticaortic aneurysm have been implicated, namely, septicembolization that usually is secondary to bacterialendocarditis; direct or lymphatic spread from anadjacent infected focus; and hematogenous seedingof the arterial wall during bacteremia from a distantfocus. In our patient’s clinical expression, in situaortic morphology and the pathohistological resultwere positive for mycotic (infective) aneurysm.The only positive microbiology result was from thepatient’s sputum for enterobacter species, which wesuppose was residual from previous pneumonia,which triggered the patient’s total inflammatorysystem response.2. Why was antifungal treatment administered?The management of mycotic aneurysms requires196 Case ReportMitrev, Z.K. et al. Mycotic Aneurysm Surgeryeradication of the source of infection and maintenanceof distal arterial flow. Surgery is almost alwaysindicated, since mortality for untreated patientsis greater than 90%. Bactericidal medicationswith a broad spectrum antibiotic and antifungalactivity should be started immediately once thediagnosis has been made. Adjustments in antibioticselection can be made following sensitivity results.Antibiotics should be continued postoperatively fora minimum of 6-8 weeks, or oral antibiotics may berequired for a lifetime, as it was in our case. Weisolated Enterococcus faecium and Candida fromthe patient’s sputum. After the third reoperation thepatient was relieved from antibiotics and antimycotics[2].3. Did you consider wrapping the anastomosiswith omentum to capitalize on the special abilityof the omentum to heal and prevent infection?No, we did not consider this due to small, but real riskof myocardial compression resulting in bulky omentaltissue occupying pericardial and/or anterior mediastinalspace, during the first and the third operationwhile the aneurysm was on the aortic arch and ascendingaorta. During the second operation, thepatient underwent life-threatening surgery, due to ruptureof the aorta, so the emergent nature of thesurgery did not allow usage of omental wrapping.Otherwise, due to hemorrhagic shock, all the tissueswere ischemic, even the patient’s omentum.



Поврзани Новости

11.06.2026
Несоница – кога сонот не е доволен за одмор
Несоницата е едно од најчестите нарушувања на спиењето и се карактеризира со тешкотии при заспивање, чести будења во текот на…
Погледни повеќе
03.06.2026
Промотивни цени – Здравјето не смее да чека
Овој јуни, во Клиничката болница „Жан Митрев“ ја ставаме превенцијата и навремената дијагностика во преден план. Овозможуваме достапност до нашите…
Погледни повеќе
04.05.2026
Успешно имплантирана првата реверзна протеза на рамо во Клиника Жан Митрев
Во Клиника Жан Митрев за првпат е успешно изведена операција со имплантација на реверзна тотална протеза на рамо, напредна хируршка…
Погледни повеќе